
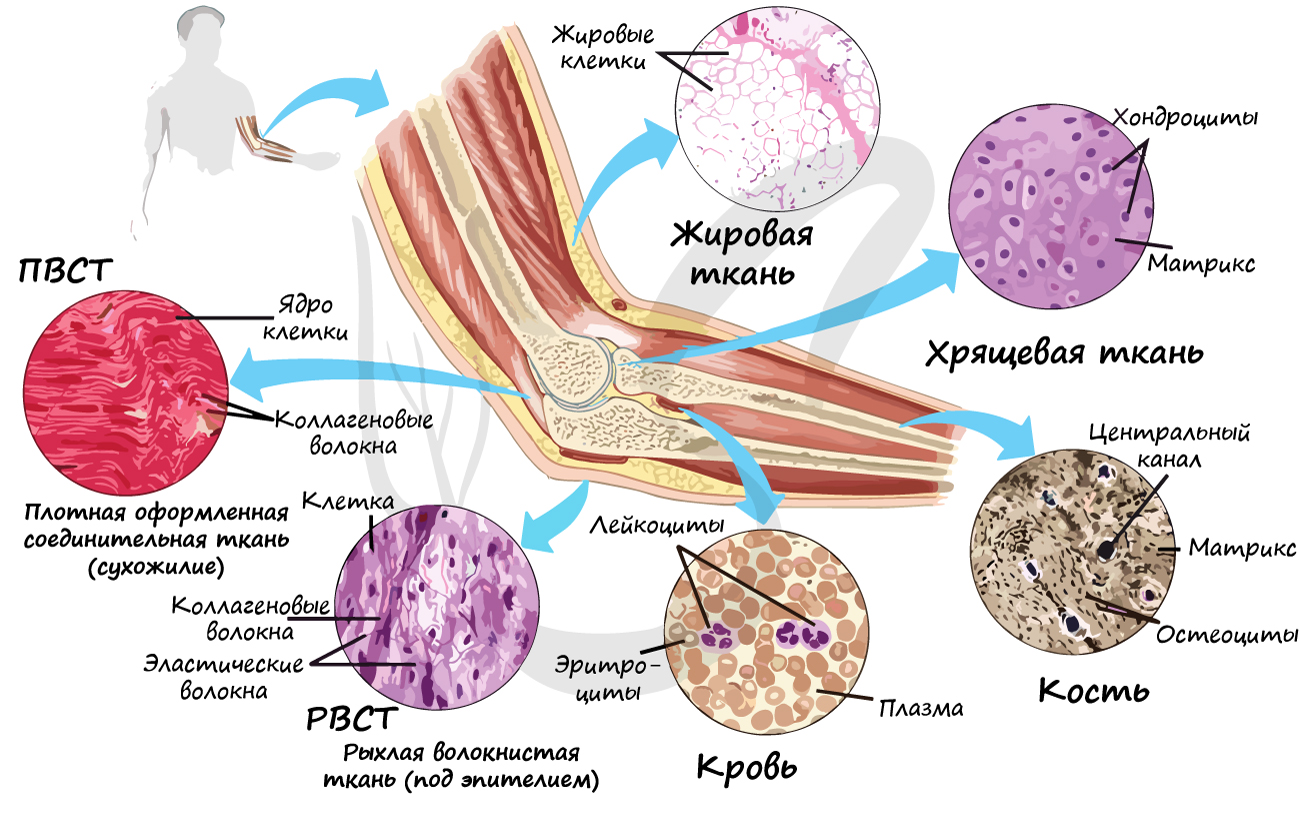
Группа соединительных тканей объединяет собственно соединительные ткани (РВСТ и ПВСТ), соединительные ткани со специальными свойствами (ретикулярная, жировая, слизистая, пигментная), скелетные соединительные ткани (хрящевая и костная). В рамках школьного курса к соединительным тканям относят жидкую подвижную кровь, строение которой мы изучим в разделе «Кровеносная система».
Что же общего между жидкой подвижной кровью и плотной неподвижной костью? Общим оказываются три основополагающих признака соединительных тканей:
- Хорошо развито межклеточное вещество
- Наличие разнообразных клеток
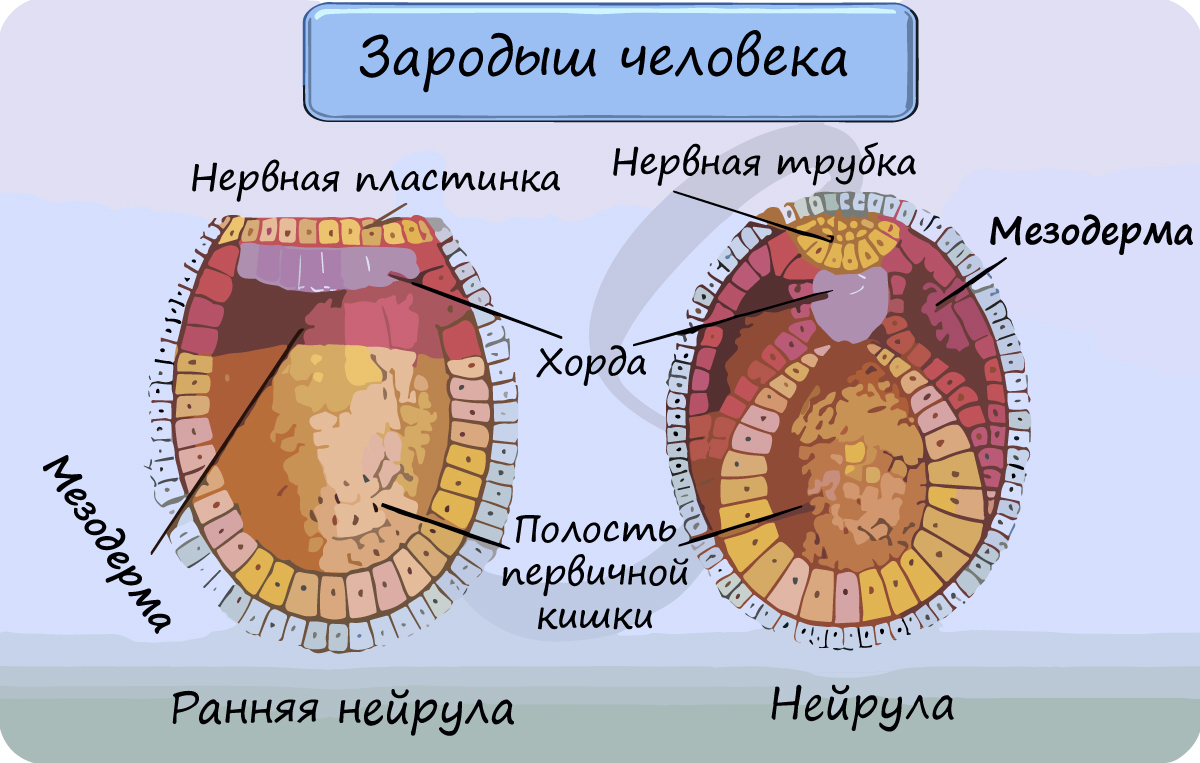
- Общее происхождение — из мезенхимы (которая развивается из мезодермы)
Межклеточное вещество соединительных тканей состоит из волокон и основного аморфного вещества (неволокнистый компонент). Волокна могут быть коллагеновыми, эластическими и ретикулярными.
Очевидно, что соединительная ткань образована тремя компонентами: клетки, волокна, основное аморфное вещество.
Собственно соединительные ткани
Собственно соединительные ткани объединяет то, что они содержат коллагеновые волокна (одни или вместе с эластическими), не отличаются высоким содержанием минеральных соединений.
Рыхлая волокнистая соединительная ткань (РВСТ) содержит клетки разной формы: фибробласты (юные), фиброциты (зрелые). РВСТ содержится во всех внутренних органах (образует строму большинства органов), она располагается по ходу прохождения кровеносных, лимфатических сосудов и нервов, образует соединительнотканные прослойки, сосочковый слой дермы.
Особенности рыхлой волокнистой соединительной ткани: преобладает основное аморфное вещество (отсюда «рыхлая», не плотная), коллагеновые и эластические волокна лежат произвольно, не ориентированы в одном направлении.
Обратите внимание на название клеток: фибробласты, фиброциты — эти слова происходят от (лат. fibra — волокно). В соединительных тканях имеются три основных типа волокон:
- Коллагеновые — обеспечивают механическую прочность
- Эластические — обуславливают гибкость тканей
- Ретикулярные — образуют ретикулярные сети, служащие основой многих органов (печень, костный мозг)

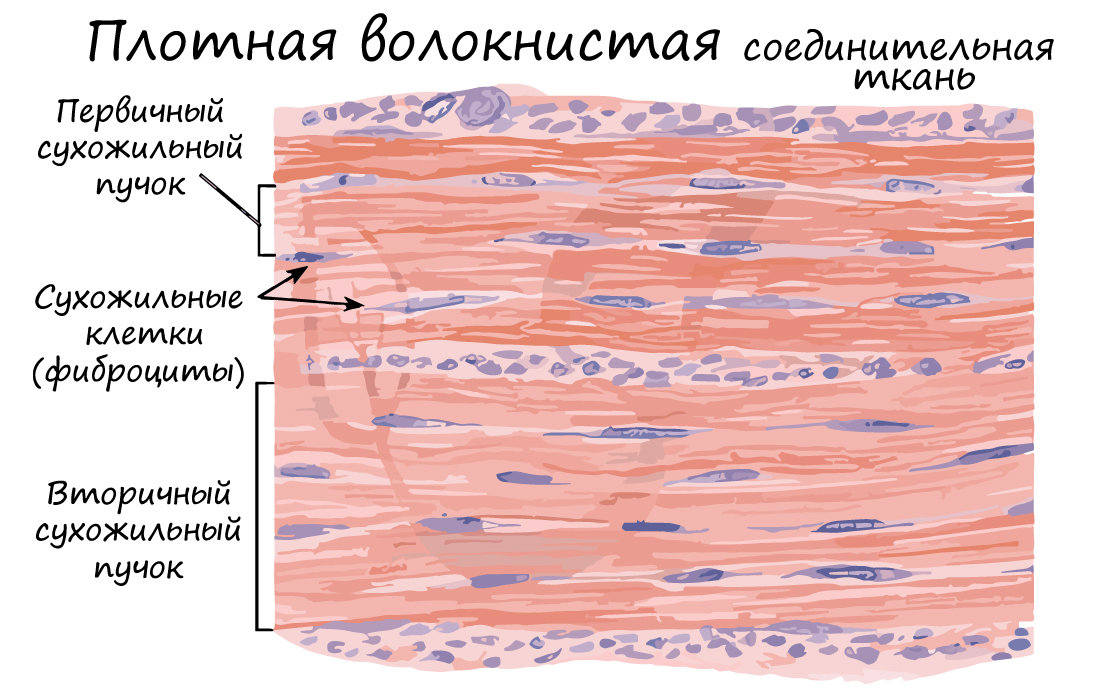
Плотная волокнистая соединительная ткань (ПВСТ) отличается преобладанием волокон (в основном коллагеновых) над клетками (отсюда термин — плотная).
Волокна могут быть ориентированы в одном направлении (оформленная ПВСТ) или нет (неоформленная ПВСТ).
Неоформленной ПВСТ образован сетчатый (глубокий) слой дермы. Оформленной ПВСТ образованы связки, сухожилия, фасции мышц, капсулы внутренних органов.
Соединительные ткани со специальными свойствами
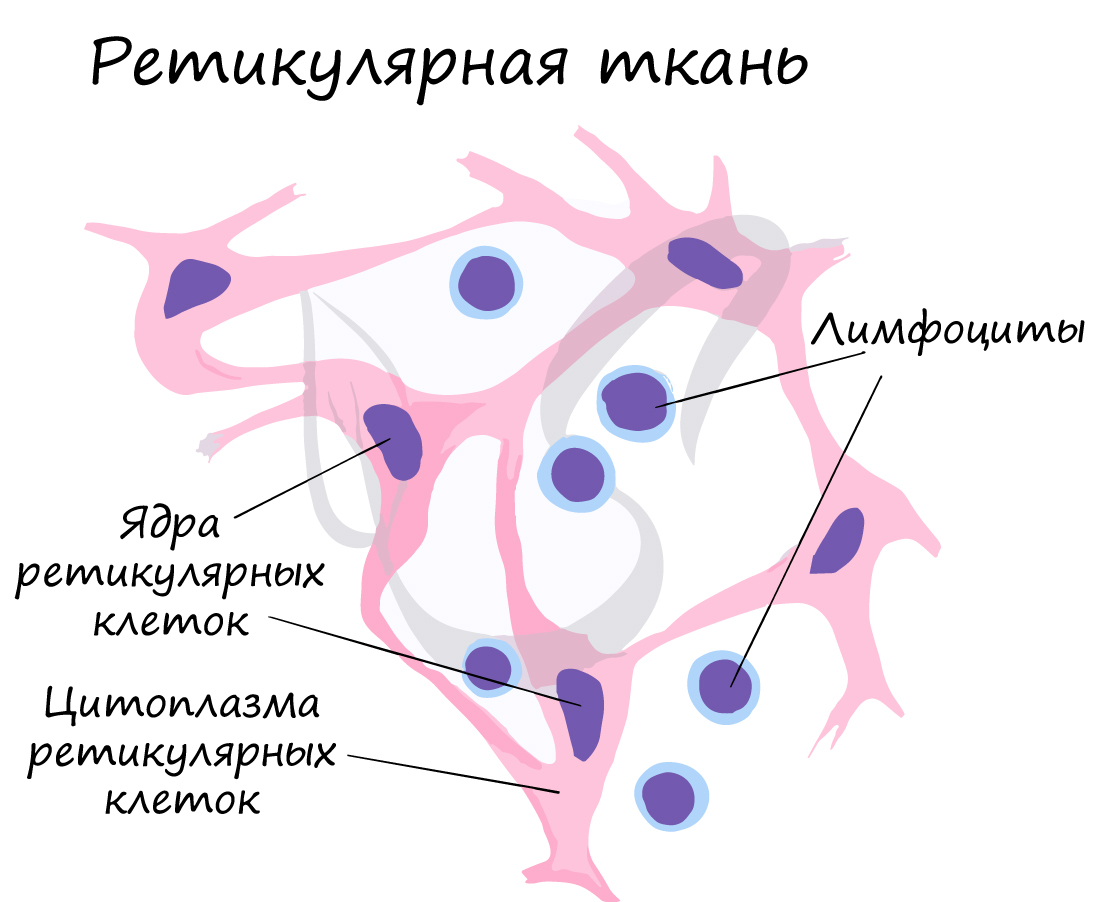
Ретикулярная ткань (от лат. reticulum — сетка) образует строму (опорную структуру) кроветворных и иммунных органов. Состоит из отростчатых ретикулярных клеток и ретикулярных волокон, объединенные в сетевидную структуру.
Ретикулярная ткань является компонентом более сложных кроветворных тканей — миелоидной и лимфоидной. Здесь зарождаются все клетки кровеносной и иммунной систем, ретикулярная ткань создает микроокружение, необходимое для такого развития.
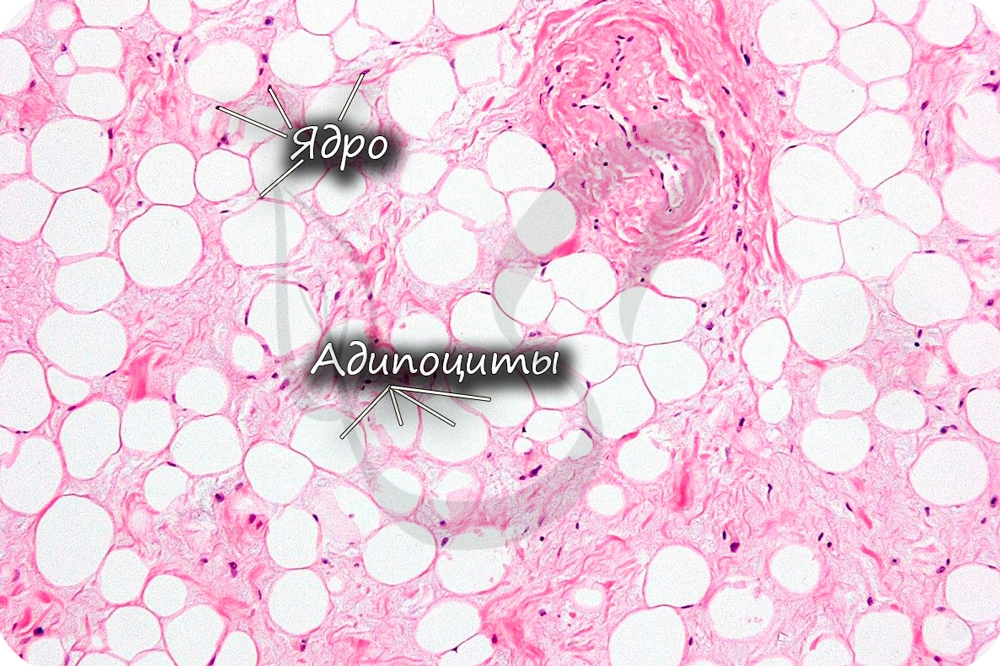
Жировая ткань состоит из скопления жировых клеток (адипоцитов — от лат. adipis — жир + cytos — клетка). Скопления адипоцитов образуют подкожную жировую клетчатку, большой и малый сальники, капсулы внутренних органов (почек), желтый костный мозг в диафизах костей.
- Жировая ткань создает резервный запас питательных веществ, накапливает жиры (липиды — от греч. lípos — жир).
- Секретирует гормоны — эстроген, лептин.
- Обеспечивает теплоизоляцию
- Предупреждает повреждения внутренних органов (защитная функция).
Слизистая (студенистая) ткань встречается в норме только между плодными оболочками и в составе пупочного канатика зародыша. Ее относят к эмбриональным тканям, на постэмбриональном этапе развития она отсутствует.

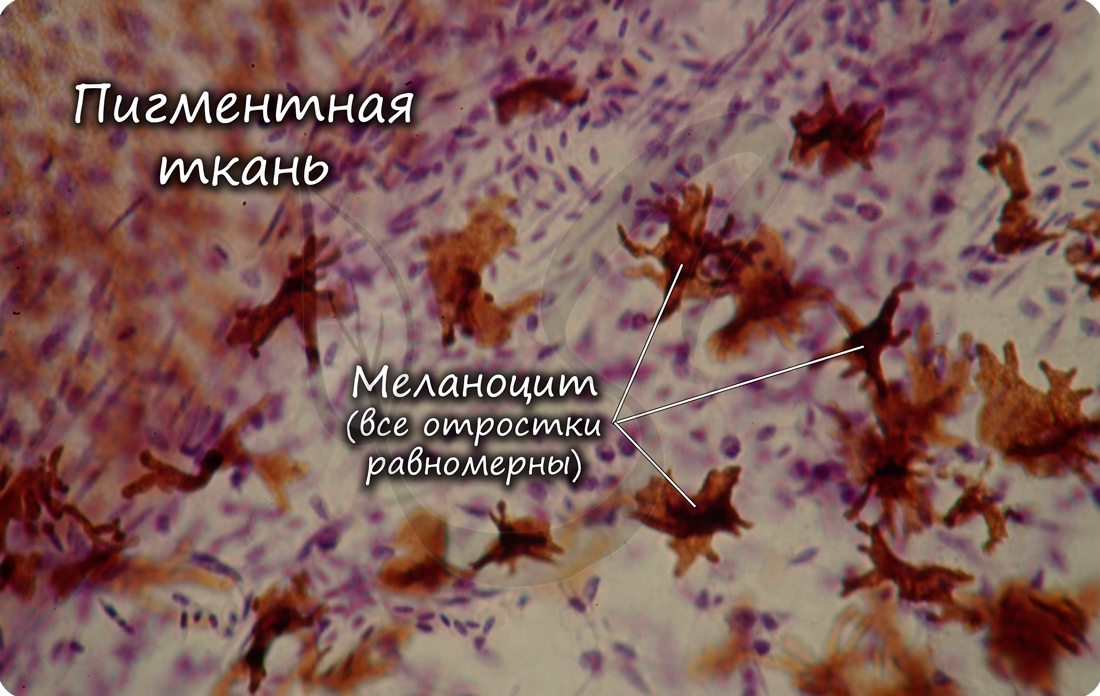
Пигментная ткань отличается большим скоплением пигментных клеток — меланоцитов (от греч. melanos — «чёрный»), развита на отдельных участках тела: в радужке глаза, вокруг сосков молочных желез.
Скелетные соединительные ткани
К скелетным тканям относятся хрящевая и костная ткани, которые создают опорно-двигательный аппарат, выполняют защитную, механическую и опорную функции, принимают активное участие в минеральном обмене (обмен кальция, фосфора). Играют формообразующую роль в процессе эмбриогенеза и постэмбрионального развития (на месте многих будущих костей вначале образуется хрящ).
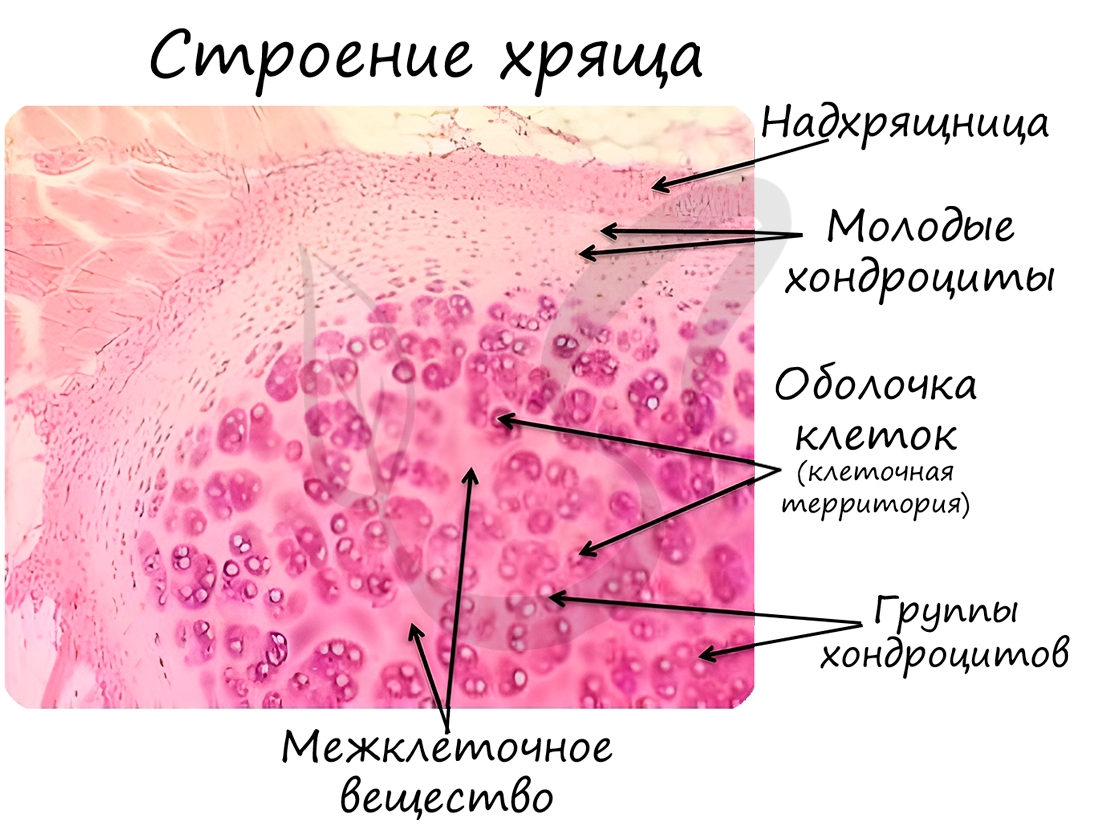
Хрящевая ткань состоит из молодых клеток — хондробластов, зрелых — хондроцитов (от греч. chondros — хрящ). Межклеточное вещество хрящевой ткани на 4-7% состоит из минеральных соединений, упругое, содержит много воды (особенно в молодом возрасте). С течением времени воды в хряще становится меньше и его функция постепенно нарушается.
В хрящевой ткани, как и в эпителии, отсутствуют кровеносные сосуды, благодаря чему хрящи отлично приживаются после пересадки. Во многих случаях хрящ покрыт надхрящницей — волокнистой соединительной тканью, которая участвует в росте и питании хряща, которое происходит диффузно.
Хрящевая ткань может быть 3 видов: гиалиновая, эластическая и волокнистая.
Гиалиновая хрящевая ткань образует суставные поверхности костей, метафизы трубчатых костей в период их роста, хрящи воздухоносных путей (гортани, трахеи и крупных бронхов), передние отделы ребер. Эластическая хрящевая ткань образует ушные раковины, хрящи носа, средних бронхов, надгортанник. Волокнистая хрящевая ткань формирует межпозвоночные диски.
Хрящевая ткань выстилает поверхность костей в месте образования суставов. При нарушении в ней обменных процессов хрящевая ткань начинает заменяться костной, что сопровождается скованностью и болезненностью движений, возникает артроз.

Костная ткань состоит из клеток и хорошо развитого межклеточного вещества, пропитанного минеральными солями (составляют около 60-70%), преобладающим из которых является фосфат кальция Ca3(PO4)2.
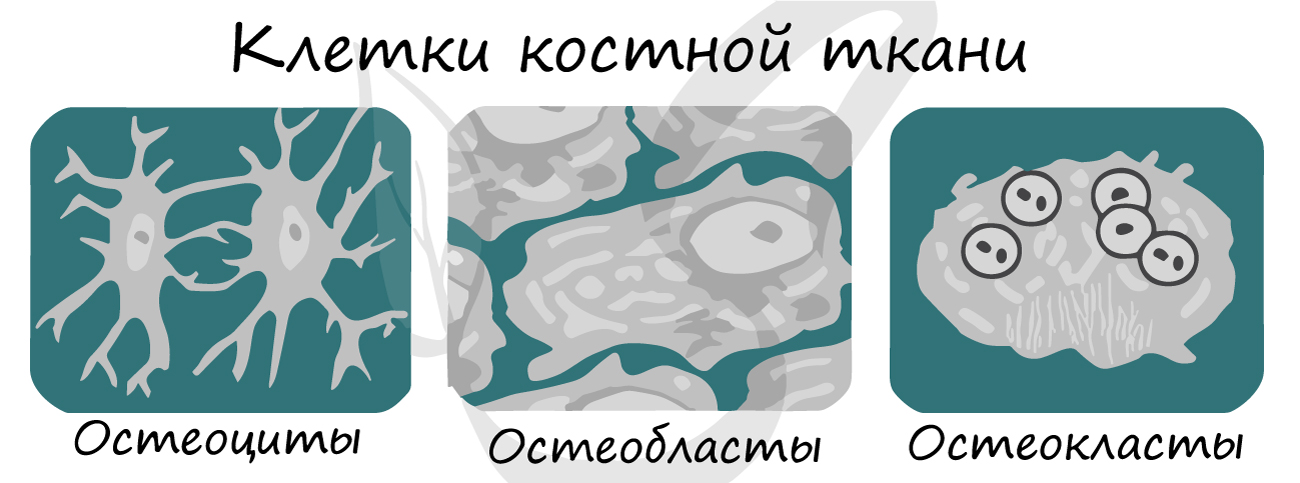
В костной ткани активно идет обмен веществ, интенсивно поглощается кислород. Кости — это вовсе не что-то безжизненное, в них постоянно появляются новые и отмирают старые клетки. В кости можно обнаружить следующие типы клеток:
- Остеобласты (др.-греч. osteo — кость) — молодые клетки
- Остеоциты — зрелые клетки (от греч. osteon — кость и греч. cytos — клетка)
- Остеокласты (от греч. klastos — разбитый на куски, раздробленны) — отвечают за обновление кости, разрушают старые клетки
Остеокласт (образуется путем слияния клеток, постклеточная структура — симпласт) — фагоцитарно активен, способен разрушать костное вещество.
Разрушение (резорбция) костной ткани — необходимая составная часть перестройки структуры кости, которая происходит в течение всей жизни.
Принципиальное отличие большинства костей от хрящей — наличие сосудов. Ткань, окружающая кость снаружи, — надкостница, содержит остеобласты и остеокласты. От сосудов надкостницы отходят многочисленные ветви, которые направляются внутрь кости и питают ее.
Кость растет в ширину за счет деления клеток надкостницы, в длину — за счет деления клеток эпифизарной пластинки (хрящевой пластинки роста).
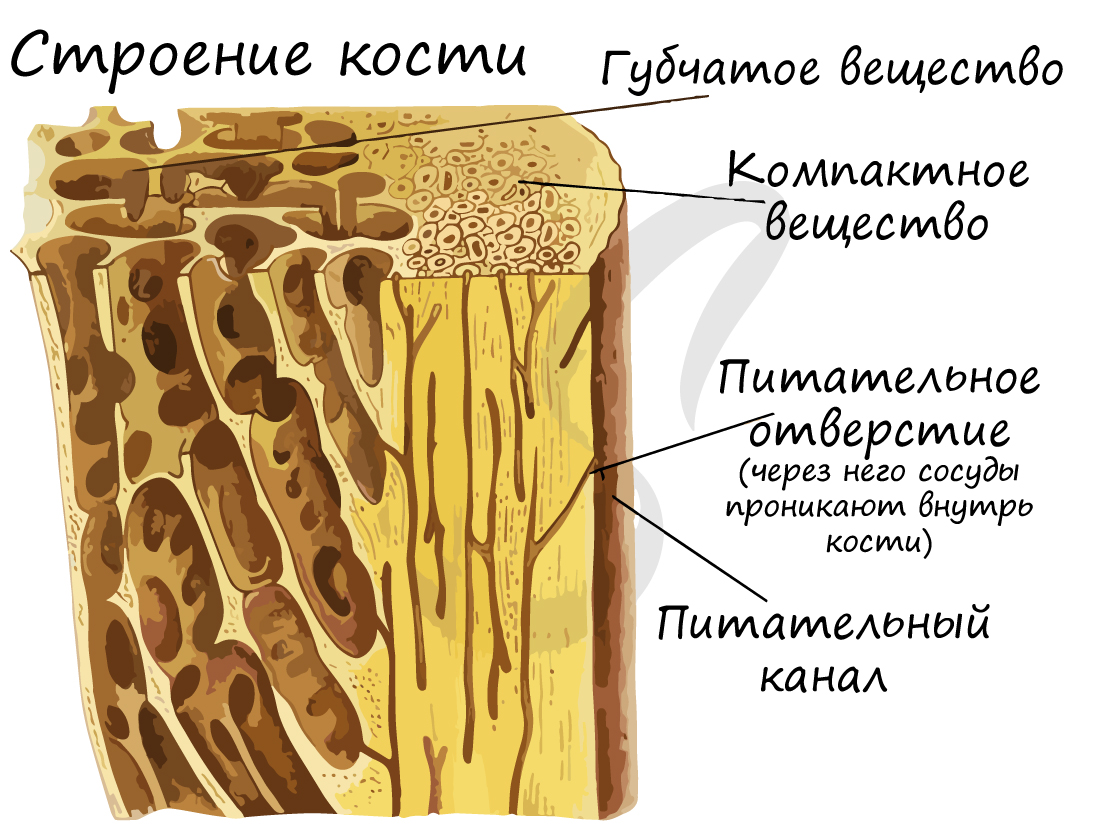
Кость состоит из компактного и губчатого вещества. Губчатое костное вещество образуют костные пластинки, которые объединяются в трабекулы (имеют форму дуг/арок). Губчатое вещество образует внутренние части губчатых и плоских костей, эпифизы трубчатых костей, внутренний слой диафиза. Содержит орган кроветворение — красный костный мозг.
Компактное вещество почти не имеет промежутков, костные пластинки имеют концентрическую форму (полые цилиндры, вложенные друг в друга). Компактное вещество образует поверхности плоских и губчатых костей, поверхностный слой эпифиза и основную часть диафиза.
Структурной единицей компактного вещества является остеон (Гаверсова система). В Гаверсовом канале, расположенном в центре остеона, проходят кровеносные сосуды — источник питания для костной ткани. По краям канала лежат юные клетки, остеобласты, и стволовые клетки. Вокруг канала лежат соединенные друг с другом остеоциты, образующие пластинки.

Кость состоит из двух компонентов:
-
Неорганический (минеральный) компонент костной ткани (60-70%)
Межклеточное вещество костной ткани содержит коллагеновые волокна, которые пропитаны минеральными солями, главным образом — фосфатом кальция Ca3(PO4)2 и кристаллами гидроксиапатита.
Минеральный компонент обеспечивает прочность кости. Благодаря нему костная ткань выполняет опорную функцию и способна выдерживать значительные нагрузки.
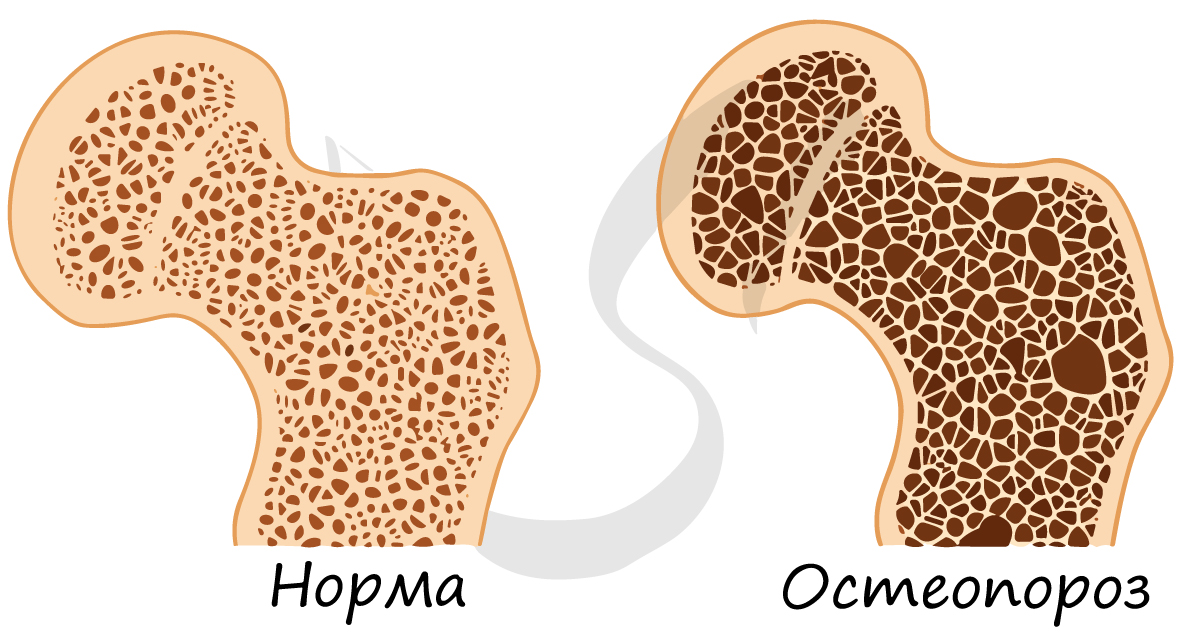
С возрастом содержание минерального компонента уменьшается (как и другого — органического компонента), в результате кость становится более ломкой и хрупкой, возникает склонность к переломам. Истончение костной ткани называется остеопороз (от греч. osteon — кость + греч. poros — пора).
Органический компонент представлен белками (коллаген — фибриллярный белок), липидами (жирами). Он обеспечивает эластичность кости — способность сопротивляться сжатию, растяжению.
Если провести мацерацию кости (химический опыт) — обработать кость сильными кислотами с целью ее деминерализации, то она станет настолько гибкой, что ее можно завязать в узел. Это возможно благодаря тому, что после опыта в костях остается только органический компонент — все соли растворяются (неорганический компонент исчезает).

Органический компонент превалирует в костях новорожденных. Их кости очень эластичные. Постепенно минеральные соли накапливаются, и кости становятся твердыми, способными выдержать значительные физические нагрузки.
Происхождение
Соединительные ткани развиваются из мезодермы — среднего зародышевого листка. Более точно — из мезенхимы, которая развивается из мезодермы.
© Беллевич Юрий Сергеевич 2018-2022
Данная статья написана Беллевичем Юрием Сергеевичем и является его интеллектуальной собственностью. Копирование, распространение (в том числе путем копирования на другие сайты и ресурсы в Интернете) или любое иное использование информации и объектов без предварительного согласия правообладателя преследуется по закону. Для получения материалов статьи и разрешения их использования, обратитесь, пожалуйста, к Беллевичу Юрию.
Dense Connective Tissue
DCT is a perfect matrix for force transmission over a distance and it creates anchors to help LCT hold tissues in place;
Related terms:
Connective and mesenchymal tissues with their stains
Dense connective tissue
Dense connective tissue is often seen as the capsules enclosing organs and, in particular, tubular structures, but is most strikingly characterized in its appearance as tendons and ligaments. These are basically dense masses of collagenic fibers and fibroblasts arranged in an orderly manner, with the cells and fibers being oriented in the same direction (i.e. parallel to the long axis of the tendon). Primarily there is a predominance of fibroblasts, but these secrete increasing amounts of collagen and the bulk of the tendon becomes fibrous. Structures of this composition possess enormous tensile strength and are perfectly suited for connecting the skeletal muscles to the skeleton and so transmitting power. Immature dense connective tissue contains capillaries, but as the fibroblasts mature to become fibrocytes and stop producing intercellular substances, the need for nutriments in quantity is much reduced and the capillary blood supply largely disappears.
Читайте также: Как сделать навес из ткани своими руками
Connective Tissues
Carla Stecco MD , . Raffaele De Caro MD , in Functional Atlas of the Human Fascial System , 2015
Dense Connective Tissue
Dense CT is characterized by large, robust collagen fibres that provide a considerable amount of strength to this tissue. Fibres are so numerous that the key identifying trait of this tissue is the absence of open spaces between cells or fibres. Since the protein fibres are the dominant component of these tissues, the types of fibres and their orientation within these tissues is the basis for the naming scheme. Dense CTs contain either collagen or elastic protein fibres; therefore, there are dense collagenous CTs and dense elastic types. The collagenous types are far more abundant and are called fibrous or ‘white’ CT. Elastic fibres, on the other hand, appear yellow in unstained tissues and are commonly referred to as ‘yellow’ CT (e.g. the yellow ligaments of the spine). Fibroblasts are the only cells visible and are arranged in rows between the fibres. Their function is to create the collagen fibres of the tissue.
The main roles of dense CT are to transmit forces over a distance and to connect different organs/muscles. Collagen fibres are disposed along the direction of mechanical loads present in that specific tissue. The capacity of dense CT to resist mechanical stress is directly related to the structural organization of the ECM and above all, the collagen fibres.
The dense CT is subclassified as follows:
Dense, irregular CT has irregularly arranged collagen fibres and usually comprises the dermis and fasciae. In the last few years, it has been demonstrated that the irregular appearance of deep fasciae may be due to its multilayered structure, but in actuality each layer presents its own regularity (see Chapter 3 ). Consequently, the deep fasciae could be classified as dense regular CT.
Dense, regular CT is a white, flexible tissue that contains tightly packed bundles of collagen fibres. All of these fibres run in one direction and are arranged parallel to the direction of forces exerted on the particular body part where the tissue is located. This arrangement is typical of tendons and ligaments, but according to recent studies ( Benetazzo et al 2011 ) the deep fasciae could also be classified in this group. Purslow (2010) demonstrated that the epimysium and perimysium have a very specific organization that also may classify them as dense, regular CT, and Huijing and Baan (2003) demonstrated this tissue’s role in force transmission (see Chapter 3 ). Finally, a specific discussion of the endomysium is necessary as it is not clear whether this has a structure similar to a microtendon ( Purslow 2010 ) or if it is better classified as loose CT ( Testut 1905 ). In the following chapters, the characteristics and functions of the deep fasciae, epimysium and perimysium will be described in greater detail.
We can further classify the regular CT according to its function:
Dense CT connecting two bones: referred to as ligaments as they are composed of collagen fibres positioned parallel to each other and rich in elastic fibres ( Fig. 1.16 ).
Dense CT connecting muscles to bones: referred to as common tendons as they are also characterized by collagen fibres positioned parallel to each other ( Figs 1.17 and 1.18 ), and there are very few elastic fibres. Tendons could be divided into two sub-categories: tubular tendons (e.g. biceps brachii tendon and patellar tendon) and flat tendons (or aponeuroses). In the past, the terms ‘fascia’ and ‘aponeurosis’ were used in an interchangeable way; however, based on their collagen fibre disposition, the aponeurosis (flat tendon type) can be differentiated from the deep muscular fascia. Both are dense, regular CTs, but aponeuroses have the collagen fibre bundles in a single direction and deep fasciae have a multilayered structure with collagen fibres disposed in a variety of directions (see Chapter 3 ). These tissues have dissimilar functions: aponeuroses connect muscles to bone and fasciae connect muscles to one another.
Dense CT connecting muscles to one another: these are referred to as deep fasciae (see Chapter 3 ) ( Fig. 1.19 )
Dense CT connecting muscle to fascia: referred to as ‘myofascial expansions’ and have their collagen fibres parallel to each other. Some expansions are flat (e.g. the lacertus fibrosus that is the expansion of the biceps brachii into the medial region of the antebrachial fascia ( Fig. 1.20 ). Other expansions could be tubular (like a tendon, e.g. the expansion of the gracilis, sartorius and semitendinosus into the crural fascia). The elastic fibres are scarce in this type of CT.
Bone- and cartilage-forming tumors and tumors of joints
Eduardo Calonje MD, DipRCPath , . Boštjan Luzar MD, PhD , in Diagnostic Atlas of Cutaneous Mesenchymal Neoplasia , 2020
Pathology
Histology
Delimited by dense connective tissue
Filled with gelatinous fluid composed of hyaluronic acid and mucopolysaccharides
Cellular lining of the cavity has features of myofibroblasts or mesenchymal cells undergoing early muscle differentiation
Immunohistochemistry/special stains
Main differential diagnoses
Low-power magnification depicting pseudocystic spaces delimited by dense connective tissue . Some of the spaces are filled with mucoid material.
Higher magnification of a fluid- and debris-filled cavity.
Another example of the entity, showing thickened pseudocyst fibrotic lining and a fluid-filled cavity.
The cells lining pseudocystic spaces are fibroblasts and myofibroblasts.
Regenerative Medicine
George C. Chang Chien DO , Agnes Stogicza MD , in Pain Care Essentials and Innovations , 2021
Ligament Pathology
Ligaments are dense connective tissue that connect bone to bone and provide stabilization to a joint. Though ligaments are functionally different from tendons as they connect bone to bone, they are structurally similar. The main differences are that ligaments have higher proteoglycan content, higher water content, lower in collagen content, and are less uniform. These structures are typically injured with supraphysiologic stretching, at the end range of motion for a joint. Acute trauma typically causes ligament abnormalities and is often marked by fluid surrounding the ligament, although chronic repetitive microtrauma may be a factor as with tendon injuries. Potential damage includes interstitial tearing of collagen fibers, partial tears that extend to the surface, and full thickness ligament ruptures. Over time, the ligament can become elongated and lax. Other evidence of injuries includes bone contusions, fractures, or joint effusion. After healing, the ligament may appear thickened, weakened, and prone to further damage. Common examples include the anterior talofibular ligament in ankle sprains and anterior cruciate ligament in knee injuries. There are limited studies investigating RM for ligamentous injuries, but there is evidence that PRP may promote the success rate of ACL repairs and provide pain relief in plantar fasciitis superior to corticosteroid. 44 , 45 Prolotherapy has been successfully used for sacroiliac joint related pain, low back pain, and coccydynia. 46–50
Toxicity and biocompatibility properties of nanocomposites for musculoskeletal tissue regeneration
4.4.4 Ligaments
Ligaments are dense connective tissues constituted by a protein phase (collagen and elastin) and a polysaccharide phase (proteoglycans). The elastic modulus of ligament is about 150–355 MPa, and the tensile strength is less than 50 MPa. Their mechanical properties are determined by the relative amount of the two phases as well as geometrical factors, conformation, and orientation of the individual constituents. Ligaments show a hierarchical structure characterized by different levels of organization, including collagen molecules, fibrils, fibril bundles, and fascicles. In recent years, artificial prostheses were used to repair or replace damaged ligaments in ligament injuries. Benefiting from nanocomposite material science and technology, poly (2-hydroxyethyl methacrylate)-based hydrogels reinforced with poly (ethylene terephthalate) (PET) fibers and PLGA scaffolds characterized by a fibrous hierarchical structure were proposed as high-performance ligament prostheses. Nanotechnology based on 3D fibrous hierarchical designs, utilizing novel braiding techniques which permit the controlled fabrication of substrates with a desired pore diameter, porosity, mechanical properties, and geometry were used to design a scaffold that provided the newly regenerating tissue a temporary site for cell attachment, proliferation, and mechanical stability. This method produces scaffolds for ligament regeneration and showed a positive result ( Ambrosio et al., 1998; Cooper et al., 2005 ). The polymer content in nanocomposites may also lead to some cytotoxicity. The specific polymers’ degradation products reduce local pH, which in turn induces an inflammatory reaction. Moreover, the rapid drop of pH in vivo may accelerate the polymer’s degradation rate, which would not be good for tissue regeneration ( Liu et al., 2006 ), such as PLGA, which can be used for ligaments and can also have this adverse effect.
Читайте также: Хлопчатобумажная ткань применяется в качестве наполнителя в винипласте
Engineering Anisotropic 2D and 3D Structures for Tendon Repair and Regeneration
Alex Lomas , . Dimitrios I. Zeugolis , in Tendon Regeneration , 2015
1 Introduction
Tendons are dense connective tissues that join muscle to bone and play a vital role in overall joint stability and function. Collagen type I fibrils are described as long crystals that are arranged in an anisotropic fashion [1–8] . These collagen fibrils are organized into primary, secondary, and tertiary bundles, responsible for the mechanical resilience of the tissue ( Table 1 ). Primary fiber bundles consist of a collection of fibrils with diameters of around 1–4 μm [9] . Secondary fiber bundles group together the subfascicles into larger units of approximately 150–1000 μm in diameter [10] , which are then grouped into tertiary fiber bundles of diameter 1000–3000 μm [11] . The diameter of the bundles is directly related to the macroscopic size of the tendon; small tendons like the flexors and extensors have small diameter bundles, while large tendons, such as the Achilles, have thicker fiber bundles [12] . Endotenon divides the bundles of collagen fibrils into areas that can be supplied with blood and nutrients. Further, endotenon is made up of a crisscross pattern of collagen types I and III and high concentrations of glycosaminoglycan (GAG) molecules that due to their water-holding capacity, allow tendon fascicles glide over each other [12] .
Table 1 . Mechanical properties of human tendons are evidently dependent on the anatomical location and the age of the patient. High load bearing tendons (e.g., Achilles) have higher ultimate strain and stress than low load bearing tendons (e.g., supraspinatus). Ultimate stress is also reduced as the age is increased
| Tendon | Patient/donor age | Ultimate load (N) | Ultimate strain (%) | Ultimate stress (MPa) | References |
|---|---|---|---|---|---|
| Achilles | 36–50 | 3534 ± 919 | 21 | 73 | [182] |
| 79–100 | 2735 ± 1371 | 22 | 48 | ||
| Rotator cuff | 28–98 | 662 ± 223 | ≥11 | 30 ± 14 | [183,184] |
| Patellar | 29–50 | 3855 ± 550 | 14 ± 6 | 65 ± 16 | [185,186] |
| 64–93 | 3346 ± 1167 | 15 ± 5 | 54 ± 10 | ||
| Extensor | 22–78 | 2914 ± 644 | 9 ± 1 | 66 ± 12 | [187] |
| Tibialis | 15–45 | 3062 ± 699 | 20 ± 5 | 127 ± 8 | [188] |
| 56–65 | 3004 ± 603 | 20 ± 6 | 111 ± 16 |
Injuries to tendons and ligaments are some of the most frequently encountered disorders presented in the clinic and can range in severity from a small sprain to complete rupture. Due to the inherent poor healing properties of tendons, injuries frequently result in long-term disability, which leads to development of degenerative disorders in later life. In USA, over 75,000 Achilles tendon ruptures, 55,000 rotator cuff injuries, and over 5 million new cases of tennis elbow are diagnosed annually, with associated health-care costs to run into the billions of dollars [13] . Tissue grafts are considered the gold standard in large tendon injuries. However, such materials have failed to restore full function due to mechanical failure at graft/tissue interface and the formation of fibrous adhesions preventing the repaired tendon from gliding correctly [14,15] . As the world population increases and ages, tendon injuries will become even more prevalent, placing a further burden on already stretched health-care systems, making the development of novel strategies to manage all types of tendon injuries and degenerative conditions imperative. To this end, anisotropic scaffolds, in form of sponges, fibers, and imprinted substrates, alone [16,17] or in combination with cells [18–20] are at the forefront of scientific and technological research and innovation for tendon repair and regeneration.
Tendon Repair
Gloria R. Sue , James Chang , in Global Reconstructive Surgery , 2019
Clinical Issues
Tendons are dense connective tissues that connect muscle to bone. Tendons transmit forces generated by muscles to move joints. Tendon injuries most commonly occur in the hand. These injuries typically result from a sharp cut or crush injury but can occasionally occur as closed injuries.
There are 12 flexor tendons in the hand and forearm. The flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) are the finger flexor tendons ( Fig. 2.3.1 ). The flexor pollicis longus (FPL) is the flexor tendon of the thumb. These flexor tendons travel beneath the transverse carpal ligament. The flexor carpi radialis (FCR), flexor carpi ulnaris (FCU), and palmaris longus (PL) are the flexors of the wrist. The PL is absent in approximately 15% to 20% of the general population.
The most intricate portions of the flexor tendons are within the digits. Here, the tendons glide within a closed fibro-osseous tendon sheath, forming a closed synovial compartment extending from the distal palm to the middle of the distal phalanx. This sheath contains an inner layer of paratenon that covers the tendons to enable smooth tendon gliding and provides nutrition to the tendon. Pulleys are intermittent fibrous condensations that exist along the tendon sheath to secure the tendon to the adjacent bone. The pulley system is an integral part of the digital flexor sheath. This unique system consists of annular pulleys and cruciate pulleys that maintain the anatomical paths of the tendons close to the phalanges to optimize mechanical efficiency of digital flexion ( Fig. 2.3.2 ). There are five annular pulleys and three cruciate pulleys. The annular pulleys are numbered from A1 through A5. The A2 and A4 pulleys, on the proximal and middle phalanges, respectively, are particularly dense and rigid. The integrity of the A2 and A4 pulleys is critical to prevent bow-stringing. The three cruciate pulleys are collapsible and allow for digital flexion to occur without significant distortion to the annular pulleys.
The FDS tendon is located superficial to the FDP proximally from the forearm to the palm ( Video 2.3.1
). At the proximal aspect of the flexor tendon sheath, the FDS bifurcates and wraps around the FDP tendon. The two slips of the FDS tendons then are rejoined deep to the FDP, forming Camper’s chiasm, at the level of the distal proximal phalanx. The FDS then inserts onto the volar middle phalanx. The FDP inserts onto the volar distal phalanx.
Injuries to the flexor tendons can be classified by zone ( Fig. 2.3.3 ). This classification system helps the surgeon assess the injury and formulate the treatment plan. Zone 1 consists of the area of the volar hand located distal to the insertion of the FDS tendon on the middle phalanx. Zone 2, also known as “no man’s land,” extends from the proximal aspect of the A1 pulley in the palm to the FDS tendon insertion. It is here where the FDS and FDP tendons interweave in a complex manner. Zone 3 covers the area from the distal aspect of the transverse carpal ligament to the proximal A1 pulley. Zone 4 is the area spanning the transverse carpal ligament. Zone 5 encompasses the area proximal to the proximal aspect of the transverse carpal ligament. The thumb has its own classification distinct from the other digits. The thumb tendon sheath consists of only the FPL tendon. Zone 1 of the thumb is the area distal to the thumb interphalangeal joint. Zone 2 consists of the area from the A1 pulley to the interphalangeal joint, and zone 3 is located over the thenar eminence.
The extensor tendons are different from the flexor tendons ( Fig. 2.3.4 ). The extensor tendons are not confined within a fibro-osseous tunnel. These tendons also become thin and flat distally over the phalanges. The extensor mechanism consists of extrinsic muscles located on the forearm, intrinsic muscles located at the level of the metacarpals, and fibrous structures. The extrinsic tendons pass through one of six distinct anatomical compartments of the extensor retinaculum on the dorsal wrist ( Fig. 2.3.5 and Video 2.3.2
). Distal to the extensor retinaculum, the extensor digitorum communis (EDC) tendons to the index, middle, ring, and small fingers are interconnected by juncturae tendinum located at the level of the metacarpals. These connections facilitate combined extension of the fingers. The index and small fingers have additional individual extensor tendons in addition to the slips from the EDC tendon. On the dorsal digits, the extensor tendons split up into a central slip and two lateral bands ( Fig. 2.3.6 ). These merge with the intrinsic extensor system to form the digital complex extensor apparatus. The central slip inserts onto the dorsal base of the middle phalanx. The conjoined lateral bands come together over the middle phalanx and continue on distally as the terminal tendon.
As with flexor tendons, injuries to the extensor tendon mechanism are classified by anatomical zone ( Fig. 2.3.7 ). Zone 1 injuries are located at the distal interphalangeal joint and distal phalanx. Zone 2 consists of the area over the middle phalanx. Zone 3 spans the proximal interphalangeal joint and includes the insertion of the central slip. Zone 4 consists of the proximal phalanx. Zone 5 is located over the metacarpophalangeal joints. Zone 6 consists of the area over the metacarpals in the dorsal hand. Zone 7 is directly over the extensor retinaculum. Zone 8 is the area between the extensor retinaculum and the musculotendinous junction. Zone 9 is located in the proximal forearm.
Solicitation of the patient’s history and the mechanism of injury provide helpful information regarding the extent of the tendon injury as well as concomitant injuries. A physical examination is critical. The natural resting posture of the injured digits is assessed for abnormalities. For example, complete laceration of both the FDP and FDS tendons is readily diagnosed when the injured digit is seen in a relatively extended position with loss of active finger flexion at the interphalangeal joints ( Fig. 2.3.8 ).
The neurovascular status of the digits should be assessed to evaluate for concomitant injury to the neurovascular bundle running along the sides of the digits ( Fig. 2.3.9 ). Emergent surgical repair is indicated in the setting of digital nerve or artery laceration. Radiographs should be obtained for open injuries to evaluate for fractures or foreign bodies.
MRI of the Kidneys and Adrenal Glands
Inflammatory Aortic Aneurysm
In IAAA, dense connective tissue infiltrated by inflammatory cells extends beyond the normal confines of the aneurysmal aortic adventitia, resulting in a periaortic enhancing rind of tissue ( Fig. 4-70 ). The periaortic tissue mantle measures up to 2 cm in thickness, and signal characteristics seem to be less predictable than the predictably prominent enhancement. 51 Prompt diagnosis and discrimination from uncomplicated abdominal aortic aneurysm ensure appropriate treatment. The presence of perianeurysmal inflammation prompts consideration of presurgical treatment with corticosteroids to minimize inflammation and operative technical modifications to minimize duodenal and ureteral dissection and improve surgical outcomes.
Postsurgical Soft Tissue Healing
Michelle M. Lesperance MS, LAT, ATC , . Brian Norton MS, ATC , in Postsurgical Orthopedic Sports Rehabilitation , 2006
Structure and Function
Cartilage is a dense connective tissue composed of chondrocytes. It provides support and structure for the skeletal system. Three types of cartilage exist: hyaline cartilage, fibrocartilage, and elastic cartilage. Hyaline cartilage, also known as articular cartilage, lines the articulating surfaces of bones and contains a high amount of collagen. Fibrocartilage is found in the intervertebral disks, as well as menisci. Elastic cartilage is found in the larynx and in the auricle of the ear, and since it has more elastin than the others, it is more flexible. Because hyaline cartilage is more frequently injured, it is discussed in greater detail.
iPSC bioprinting for musculoskeletal tissue
S. Romanazzo , . I. Roohani , in iPSCs in Tissue Engineering , 2021
Bioprinting for cartilage tissue
Cartilage is a dense connective tissue with heterogeneous mechanical and biological properties, due to the highly organized ECM consisting predominately of proteoglycans (GAG) and collagens. Current clinical treatment strategies and tissue engineering approaches have been unable to recreate the complexity of natural (e.g., hyaline) cartilage.
Earliest studies on cartilage bioprinting were conducted almost a decade ago, where chondrocytes were bioprinted in alginate ( Schuurman et al., 2011 ) or poly(ethylene glycol) dimethacrylate (PEGDMA) ( Cui et al., 2012 ). Subsequently other biomaterials, either naturally available, such as agarose or collagen, or synthetic materials, such as PCL, PLA, PEGDA, GelMA, and PEG, have been tested for the fabrication of cartilage engineered tissues. PCL and PLA hold great mechanical property and biocompatibility; however, the high temperature at which they need to be processed for printing make them unsuitable for bioprinting. To overcome this issue, hybrid constructs, where a skeleton of PCL is combined with cell-laden hydrogels, have shown promising outcome ( Daly et al., 2016 ).
Abbadessa et al. synthetized a methacrylated chondroitin sulfate (CSMA) hydrogel and used it for printing constructs with tailorable porosity and good biomaterial handling properties. In addition, chondrocyte cells showed high viability (94 ± 5%) and proliferation ability when kept in culture for up to 6 days post-printing ( Abbadessa et al., 2016 ).
Shim et al. used a custom-designed 3D printer multi head tissue/organ building system (MtoBS) to print a multilayered construct that would mimic osteochondral tissue. they used four printheads for: (i) PCL, (ii) cell-laden pepsin-treated collagen (atelocollagen) hydrogel with BMP-2 incorporated, for the subchondral bone layer, (iii) cell laden hydrogel composed of cucurbit[6]uril (CB[6])-HA (5%w/v) with TGF-β for superficial cartilage layer and (iv) 1,6-diaminohexane (DAH)-conjugated HA (DAH-HA) (5% w/v). CB[6] is a synthetic molecule that allows noncovalent cross-linking with HA ( Fig. 9.3 ). For this study human turbinate-derived mesenchymal stromal cells (hTMSCs) were used. When 3D printed samples were implanted into rabbit knee joints, they showed neocartilage formation, osteochondral integration, and a smooth cartilage cap in the area of the defect ( Shim et al., 2016 ).

Figure 9.3 . Bioprinting for cartilage and bone tissues. (A) 3D printer multihead tissue/organ building system (MtoBS), ( Shim et al., 2016 ), (B) iPSCs embedded in cellulose/alginate (NFC/A) ( Nguyen et al., 2017 ), (C) ( Cui et al., 2012 ), (D) ( Zhu et al., 2018 ), (E) ( Daly et al., 2016 ).
(A) adopted with permission, copyright (2016) IOP Publishing; (B) copyright (2017) Springer Nature; (C) copyright (2012) Mary Ann Liebert; (D) copyright (2018) IOP Publishing; (E) copyright (2016) IOP Publishing.
Cartilage tissue is among the few tissue types that have been developed with iPSC bioprinting techniques. In 2017, Nguyen et al. showed the very first cartilage TE construct developed by bioprinting undifferentiated iPSCs. They embedded hiPSCs derived from patients’ chondrocytes in either nanofibrillated cellulose/alginate (NFC/A) or NFC/HA hydrogels with different material ratio. NFC/A ratio of 60/40 showed the best iPSC viability and expression of collagen type II after 5 weeks post-printing. iPSC were also coprinted with irradiated chondrocytes to help their differentiation toward cartilage. From the experimental results, NFC/A bioinks appeared to be the most suitable for bioprinting iPSCs to support cartilage production in coculture with irradiated chondrocytes ( Nguyen et al., 2017 ).
A recent study from Kim et al. showed a prototype of artificial trachea with mechanical properties similar to the native trachea and with regeneration capabilities of tracheal mucosa and cartilage. They developed a bilayered scaffold consisting of an electrospun PCL as inner layer and a 3D printed PCL scaffold as the outer layer. iPSC-derived chondrocytes encapsulated in Matrigel, iPSC-MSCs, and human bronchial epithelial cells were then seeded on the outer and inner layers post-printing. When implanted into a segmental trachea defect of a rabbit model, iPSC-MSCs implanted showed to differentiate and form ciliated columnar epithelium and iPSC-derived chondrocytes were able to form neocartilage tissue ( Kim et al., 2020 ).
- Свежие записи
- Балкон в многоквартирном доме: является ли он общедомовым имуществом?
- Штраф за остекление балкона в 2022: что это и как избежать наказания
- Штраф за мусор с балкона: сколько заплатить за выбрасывание окурков
- Оформление балконного окна: выбираем шторы из органзы
- Как выбрать идеальные шторы для маленькой кухни с балконом